
‘Tis the season of health in U.S. and the mood is not healthy. Open enrollment periods in ACA (‘Obamacare’), fears about repeal of Obamacare by the new U.S. administration, and consequently, media and personal finance blogs worrying about impact of impending changes on the cost of health insurance and even the viability of early retirement. In addition, it is generally known that U.S. has one of the least efficient healthcare systems in the world.
All this is bound to become a serious Thanksgiving dinner topic..try to avoid food fights at the table. 🙂
In this scenario, I don’t want to further add to the grumble about the uncertain future of healthcare in U.S. Here at Ten Factorial Rocks, we want to give you a different food for thought (By ‘we’, I am including Mrs. TFR for bringing a great example to this discussion). We would like to offer you a shining example of why healthcare is affordable and better in some parts of the developing world.
Healthcare Without Borders
Cheaper I know, you say, but better? Yes. Healthcare is a complex subject and the quality of care is not correlated to cost as strongly as you may think. The case in this article will make you think why U.S or even U.K. and similar Western countries that have nationalized healthcare are dealing with the twin burden of increasing costs with unsatisfactory health outcomes.
All FIRE aspirants must understand this topic well, for protecting our health without losing our hard-earned wealth.
As my friend Physician on FIRE might say, healthcare is an umbrella term for various highly specialized subjects, with each specialty having its own nuances. Each specialty of healthcare should do its own introspection of why one country’s system is better than another. If I have to cover every medical specialty in one article, this will actually become a book. I don’t have the time and you probably don’t have the patience for reading it! Medicine is normally not a topic of personal finance, but it deeply affects the quality of our life and even the reality of financial independence.
By this illustrative case study, you can see from both real-life experience and substantive results that it is possible to have affordable and quality health care (the two words are not necessarily opposed). Much like how Henry Ford’s assembly line revolutionized manufacturing and brought high quality and affordable automobiles to all, there are similar principles that can be applied to make affordable, high quality healthcare a reality.
Case: Miracle in Ophthalmology

Visionary eye care
This case study is focused on eye care (ophthalmology). In future posts, I will cover other specialties like cardiology and orthopedics. I am using this example to show how a healthcare network in India is showing the world that it is possible to deliver top quality ophthalmic care at a fraction of the cost in developed economies. The case study is from a report which uses U.K. as the benchmark, and U.K. has nationalized health care (NHS, as the British call it), which is comparatively lower in costs than U.S. where the individual consumers and private insurance companies pay bulk of the costs.
The institution I am referring to is Aravind Eye Care System, which operates mostly out of South India. I have personally visited their facilities, and while they are not swanky like a U.S. hospital, they are spartan and clean. In this article are three charts that will blow your mind, as they did mine, on what Aravind delivers every day.
Click to enlarge
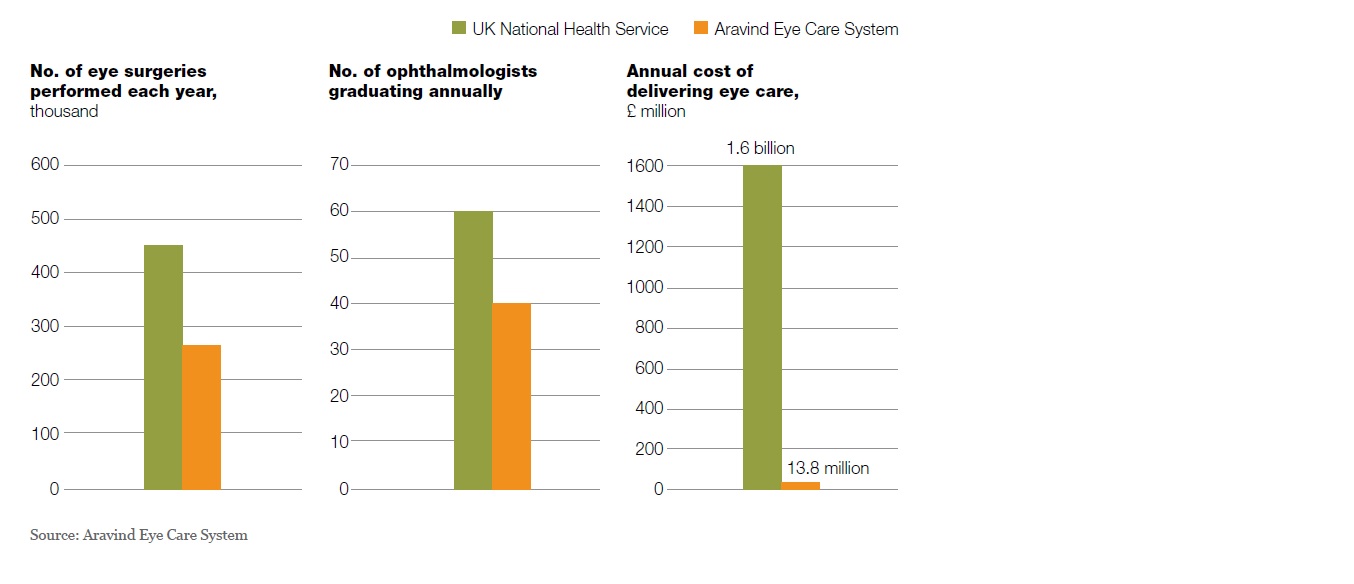
Aravind does over 260,000 eye surgeries a year, compared to 550,000 eye surgeries in all of U.K. done through the NHS system. Just one eye care institution in India (a country that has many such eye care specialist hospitals) doing more than half of U.K’s total eye surgeries is amazing in itself. What’s more amazing is that these surgeries, collectively, cost only £13.8 million ($17.2 million) versus £1.6 billion (~$2 billion) in U.K. You divide this by number of surgeries and you get Aravind’s average cost per eye surgery is only $66 versus $3600 in U.K! In the U.S, the average cost would be twice or more than U.K’s figures.
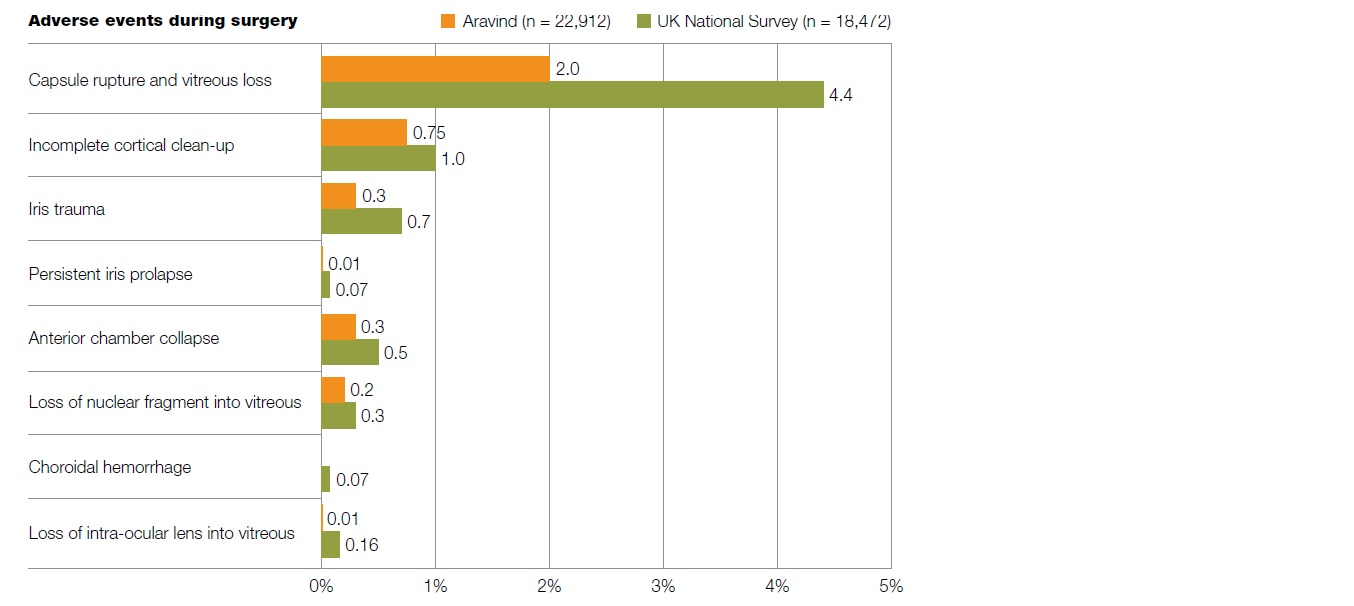
Before you imagine a caveman with a hot needle poking one eye and then yelling ‘Next!’, let me assure you that the quality of care from Aravind is top notch as the results bear out. Data (from about 23,000 randomly chosen patients) show much lower level of surgical complications from Aravind compared to UK National Survey. This covers just about every adverse event during eye surgery. See the impressive chart below.
Click to enlarge
How do they do it?
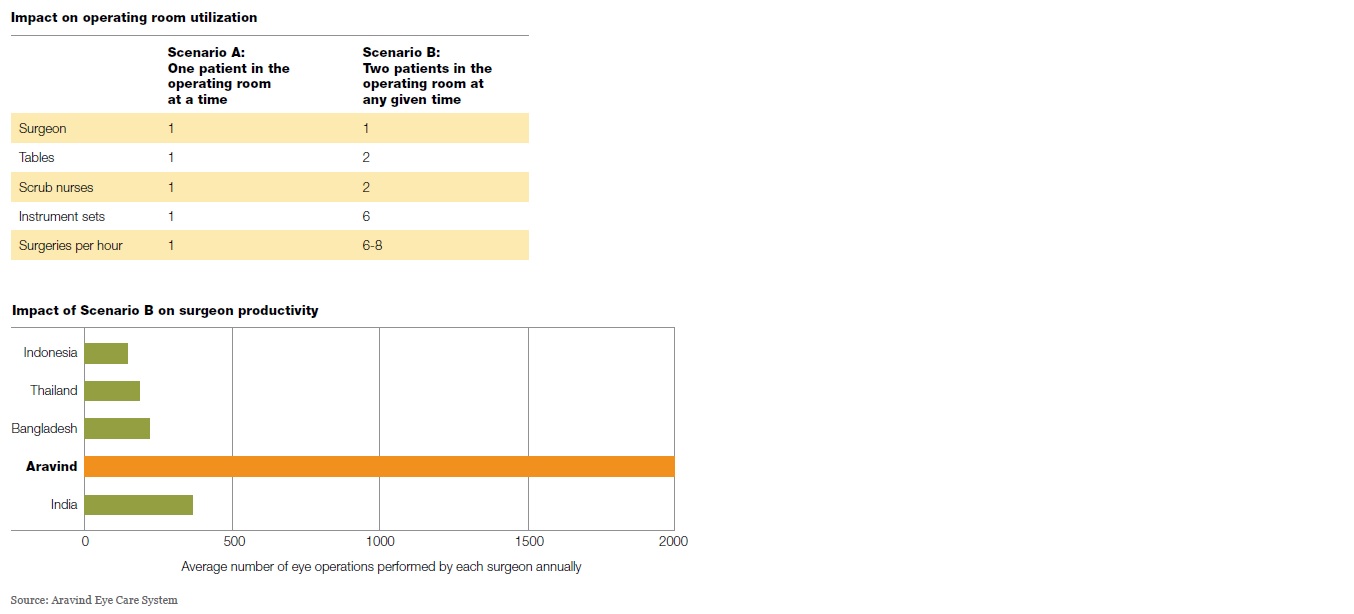
A big part of Aravind’s success is their ‘assembly’ model where they believe that each person in the healthcare chain should focus exclusively on their specialty and nothing else. For example, an ophthalmic surgeon only does the core surgery and is not involved in pre-op, post-op care and also not involved at all in any paperwork. Even the pre-op counseling is done by another doctor. They also have more nurses and ‘attendants’ per doctor than the western health systems. They pioneered the concept of having more than one patient in the operating room, so while one is getting operated on, others are getting prepped up for surgery. This happens like clockwork.
Click to enlarge
A surgeon I talked to put it this way:
“All I do is surgery, all day and everyday. I spend only few minutes per patient. I trust the people before and after my station to handle everything else. If I can do 25-30 surgeries in a day when a doctor in the U.K. or U.S. does 2-4, you shouldn’t be surprised why our clinical outcomes are better. Surgery is a skill that improves with practice and I get plenty of practice every day. I have seen just about every patient physiology with a wide range of vitals. In just one month here, I get a year’s worth of surgical experience I can get in an American hospital”.
I emphasized the word ‘station’ as we normally hear this in an assembly line. Another doctor actually cited Ford’s assembly plant and McDonald’s operations as examples of consistent quality at very low cost. That principle, he said, applies to healthcare as well. It also helps that the doctors hardly pay any insurance (other than periodic license fees and re-certifications). Malpractice insurance is a burden largely unique in U.S. My U.S. based physician friend says this drives up cost and also, encourages cover-your-ass tests and processes that may not help outcomes.
Another thing that drives these doctors is their ‘mission’ orientation. These doctors sure can get paid far more in for-profit hospitals but they choose to work in Aravind for the tangible social impact, respect they get and enduring satisfaction. They also collaborate with leading healthcare research centers in the world and admit doctoral students and residents for projects to continually drive down cost of care while improving outcomes.
Aravind also has a stated mission of preventing ‘needless blindness’. They say every incoming patient (and there are many people from different parts of India and the world who get their eye surgeries done in Aravind) subsidizes a poor patient in India. They openly practice a tiered system of fees and also, accept donations. There is no difference in the surgeries they do but in the way the patients are accommodated (subsidized patients are housed in a dormitory of sorts with a basic bed while the others get to recuperate in plush private rooms). The system works for everyone.
There are many lessons Americans can take from such successful healthcare providers in the developing world. However, it requires the entire eco-system to change to put affordability and quality where it matters as the main goals and everything else as secondary.
*************************
Added Later: Full time finance (FTF) commented below to consider purchasing power parity (PPP) in the analysis. This is a valid point for making cost comparisons of goods and services across international borders. According to World Bank, PPP of Indian Rupee to USD is 17.12 (2014 figures, cited in this article). PPP considers the wage, tax and material cost differential across countries that collectively determine how much a product or service is priced and adjusts for all this, making cross-border comparisons easy. See example below for cataract surgery.
Actual Cost of Cataract Surgery in Aravind (per eye, including internationally produced aspheric lens): INR 8750 (~$125)
PPP-adjusted cost in USD: $511 (8750 / 17.12)
US average cost of Cataract Surgery (no insurance/medicare): $3,542
It costs 593% more (7 times) in U.S. even in PPP-adjusted terms for the same cataract surgery compared to Aravind.
In real terms, the cost is 28 times higher in U.S.. This is the actual benefit a FIREd person will realize because the $511 PPP is purely for economic analysis across countries and not what you actually pay. You pay only $125. That’s why this is affordable to many Indians as well and they have no insurance – more than 90% of Aravind’s patients are Indian. The small minority of international patients are major beneficiaries as the 28X cost savings factor applies to them.
Raman Venkatesh is the founder of Ten Factorial Rocks. Raman is a ‘Gen X’ corporate executive in his mid 40’s. In addition to having a Ph.D. in engineering, he has worked in almost all continents of the world. Ten Factorial Rocks (TFR) was created to chronicle his journey towards retirement while sharing his views on the absurdities and pitfalls along the way. The name was taken from the mathematical function 10! (ten factorial) which is equal to 10 x 9 x 8 x 7 x 6 x 5 x 4 x 3 x 2 x 1 = 3,628,800.
14 comments on “Affordable & Better Healthcare: It is Visionary”